
Abdominal Aortic Aneurysm
Copyright 2007
Ashley Davidoff MD
An abdominal aortic aneyurysm (AAA) is a focal widening of all three mural layers of the abdominal aorta, usually considered when the transverse dimension of the aorta is greater than 3 cm. , or 1.5 times it’s normal diameter.
HISTORICAL First surgical repair Dubost 1952
Causative Factors
Factors that cause and predispose to aneurysmal disease include the atherosclerotic process, with associated inflammatory and degenerative changes of the aortic wall. The degenerative changes in the matrix of the aortic wall occur with age, proteolysis, and inflammation induced by the atherosclerotic process, Circulating proteolytic activity results in an increase in the elastase in the aortic wall and a subsequent breakdown of the elastin. In COPD there is increased elastase activity as well resullting in increased elastolysis. AAA is more commonly seen in males over 60 years, with a M:F ratio of 5:1. The incidence in Western cultures has tripled over the last 3 decades, due to the larger numbers of people in the elderly population. Improved diagnostic techniques have also been a major factor in the apparent increased incidence. In the USA, AAA is 13th in the leading causes of death. Only about 50% percent of patients survive a ruptured abdominal aorta. Other factors that contribute to the development of aneurysmal disease of the abdominal aorta include smoking, hypertension and familial factors. 90 percent of patients with aneurysms have a smoking history and 60% have hypertension – (Pokrovskii ) Asociated diseases include coronary artery disease and peripheral vascular disease. 90% of patients with AAA have CAD (Pokrovskii )
Statistics
5 percent of men older than 65 years of age will have an occult aneurysm (3 to 6 cm in diameter). 15,000 deaths per year are directly attributable to an abdominal aortic aneurysm, making it the 13th leading cause of death in the United States. AAA account for 95% of all aneurysms. M:F 4:1 peak incidence men occurs in men >80 and women >90 The incidence in patients <60 years is less than 1%
Associated Diseases
Common iliac artery aneurysms 20%(Armon) Popliteal aneurysms 8-10% (Ebaugh,MacSweeney) Common femoral artery aneurysms association COPD
Pathogenesis
Law of Laplace Tension = radius X pressure/wall thickness RESULTS: In most instances (90%), AAA is infrarenal and the aneurysm extends into the iliac arteries in about 2/3 of the patients. Rupture occurs in 25% of patients. Factors that predispose to aneurysmal rupture include large aneurysm size, presence of hypertension and chronic obstructive pulmonary disease (COPD). Complications: Size vs risk of rupture 4cms <5%/year 5cms 5 – 10% per year 7cms 15-25% per year 8cms 25-40% per year >9cms 75% per year Dx 75% of patients with an AAA are asymptomatic. Symptoms include abdominal pain or tenderness, back pain. Aneurysms become palpable when they are larger than 4 cm in diameter. The aneurysm is commonly identified on plain film and is easier seen on a lateral abdominal film, since 90% have mural calcification. However AAA are evaluated by their transverse dimension which cannot be measured on a lateral examination.
Diagnosis
Imaging
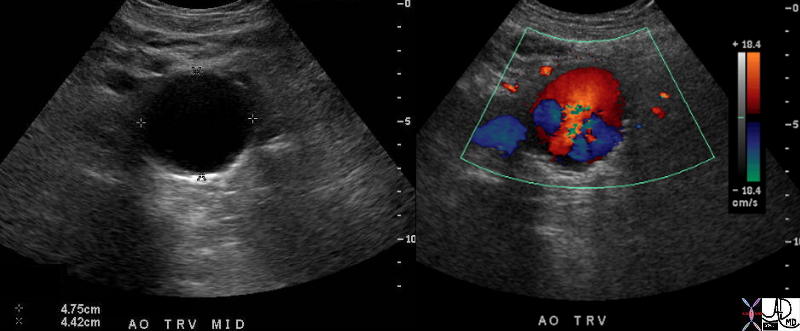
Turbulence in an Abdominal Aortic Aneurysm |
| 37669c01 aorta abdomen abdominal aort AAA enlarged aneurysm abdominal aortic aneurysm turbulent flow USscan color flow doppler Courtesy Ashley Davidoff MD |

Smooth Narrowing of the Lumen Due to Aneurysmal Disease |
| This angiogram of the abdominal aorta (a) and iliac arteries (b), shows an unusually straight and narrowed infrarenal aorta indicative of thrombus in the wall of an abdominal aortic aneurysm. In addition there is an aneurysm of the right common iliac artery and a subtotal occlusion of the left common iliac artery. Note the left kidney is small and there is a wedge shaped defect in the upper and lateral aspect of the kidney indicative of an infarct, probably embolic in origin. Courtesy Laura Feldman MD. 36005c code abdominal aorta aneurysm artery iliac stenosis occlusion kidney infarct wedge embolus |
Screening?
>60 M clinical (20-90% sensitivity) US 90-97% (sensitivity) reasonale for high risk men >60 hypertension, claudication, family history, or other vascular disease
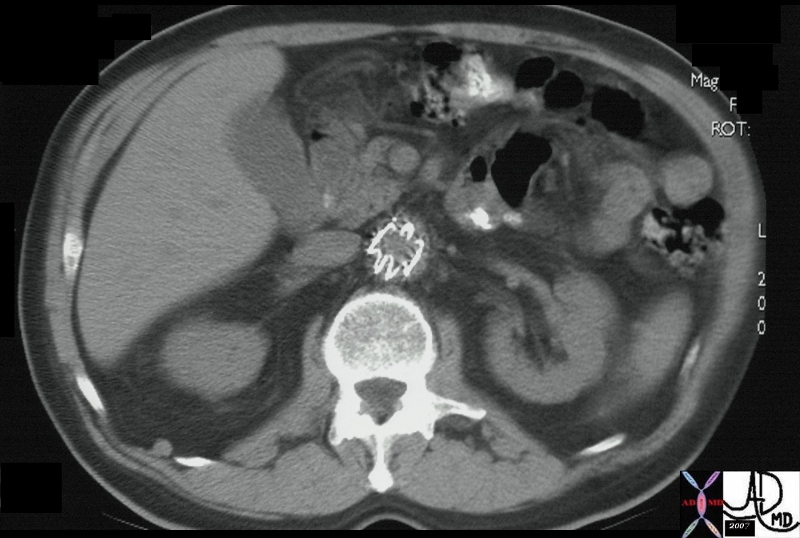
CTscan
CTA is the most commonly utilised method of evaluation since surgical questions relating to size, and position of the aneurysm with reference to the renal and iliac arteries can be answered.
US
AAA are best followed by US at 6 monthly intervals. US has an accuracy of 98% in asessment of the size of the AAA. Angiography, once the gold standard is rarely used for diagnostic purposes. The transverse size of the aorta is the measurement that is used for evaluation. The aorta is considered aneurysmal, when the transverse diameter is greater than 3cms or when a true cross sectional diameter at any level is greater than 1.5 times that of the smallest diameter. Surgery is considered when the size reaches 5cms although in some centers 4cms is the cut off. Rapid expansion is an indication for surgery and is considered when the diameter increases by more than 0.5 cm over 6 months. BAck pain in a patient with a known aneurysm is strong indication for surgery.
Protocol for Imaging Follow Up
Ultrasound for aorta < 5 cm (by ultrasound)
Aortic dimension 2.5 -3.4cms – repeat ultrasound in 5 years
Aortic dimension 3.5-3.9cms – repeat ultrasound in 2 years
Aortic dimension 4- 5 cm – repeat ultrasound in q6 months
Aortic dimension 5-5.4 cm – repeat ultrasound in q3 months and do a planning CTangio with contrast
Aortic dimension >5.5cms – elective surgery
Aortic dimension >8cms – admit the patient
Indications for Surgery
Surgery is indicated for aorta 5.5 cm or larger Aneurysmal rupture usually occurs when the aneurysm enlarges to greater than 6 cms. The rupture rate at 5 years for an aneurysm 7 cm or more in diameter exceeds 75%. For aneurysms 6 cm in diameter, the rate is about 35%, and for those 5 to 5.9 cm in diameter, it is about 25%. At this time, data are insufficient to accurately estimate the risk of rupture in aneurysms less than 5 cm (2 in.) in diameter. RX Indications for surgical intervention include an aneurysm greater than 5cms, back pain related to the aneurysm or rapid growth of the aneurysm (enlarging 0.5 cm in 6 months). Both conventional surgery as well as endovascular stent-graft placement can be used in the treatment. Gold standard is surgery with graft patency at 5 years of 90% Mortality for elective surgery is 2%, for the AAA that is symptomatic it is 20% and for the ruptured AAA it is 50%. Graft material dacron or ePTFE Indications for endovascular stent graft High risk for surgery Infrarenal neck 1cms-2.8cms Other considerations relate to the landing sites which include iliac tortuosity and size.
Management: Elective Surgical Repair Indications Aortic aneurysm diameter >=5.5 cm AAA diameter 4-5 cm and enlarging 0.5 cm in 6 months
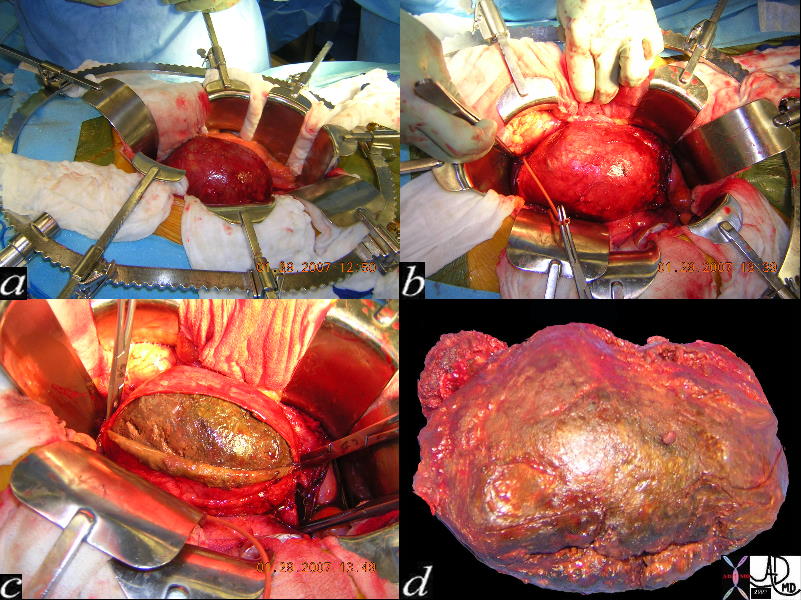
Thrombus Remioved from a AAA |
| 72460c02 aorta AAA abdomen abdominal aortic aneurysm 12 cms aneurysm surgical exposure retractors surgical exposure control upper inflow with cross clamp control of outflow opening the aoric wall exposing the lumen filled with thrombus operating room treatment Courtesy Syed Razvi MD |
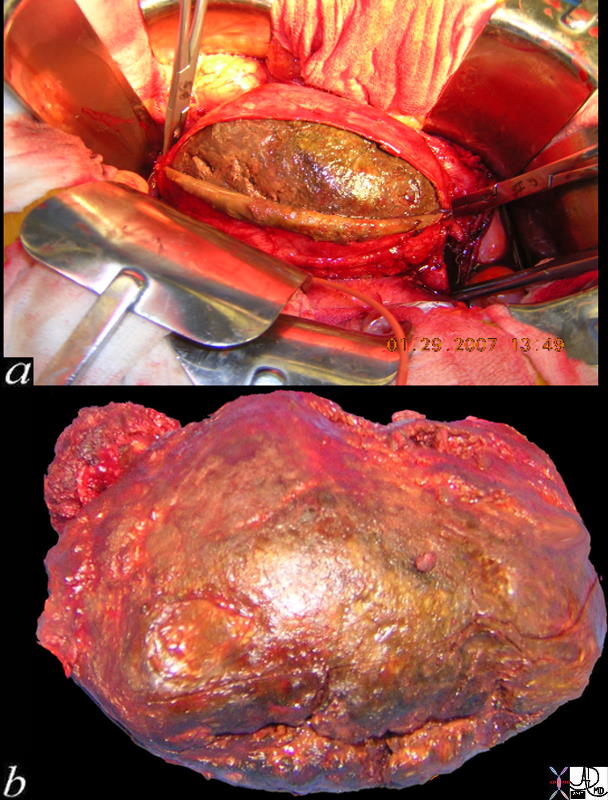
Thrombus Remioved from a AAA |
| 72460c01 aorta AAA abdomen abdominal aortic aneurysm 12 cms aneurysm surgical exposure retractors surgical exposure control upper inflow with cross clamp control of outflow opening the aoric wall exposing the lumen filled with thrombus operating room treatment Courtesy Syed Razvi MD |

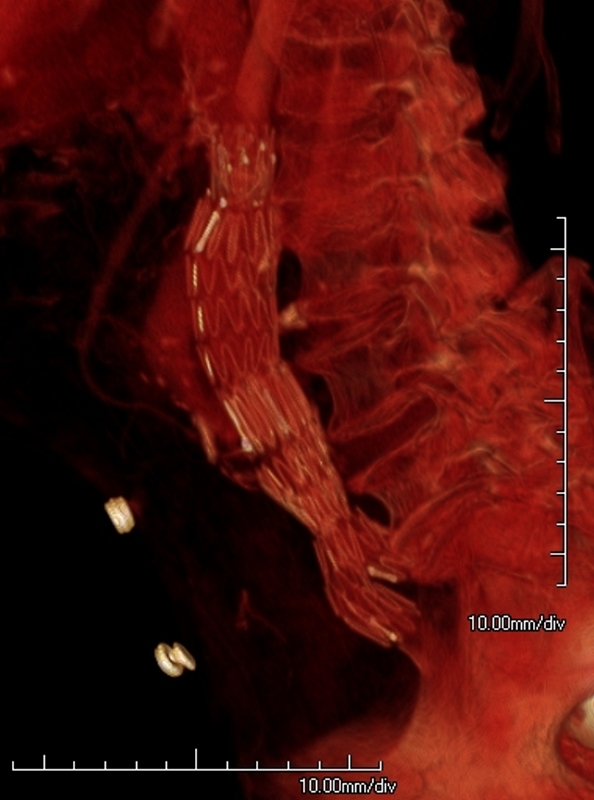
Stent Graft for Abdominal Aneurysm |
| 24284b01 aorta AAA repair abdominal aortic aneurysm MIT stent graft X-ray plain film KUB Davidoff MD |
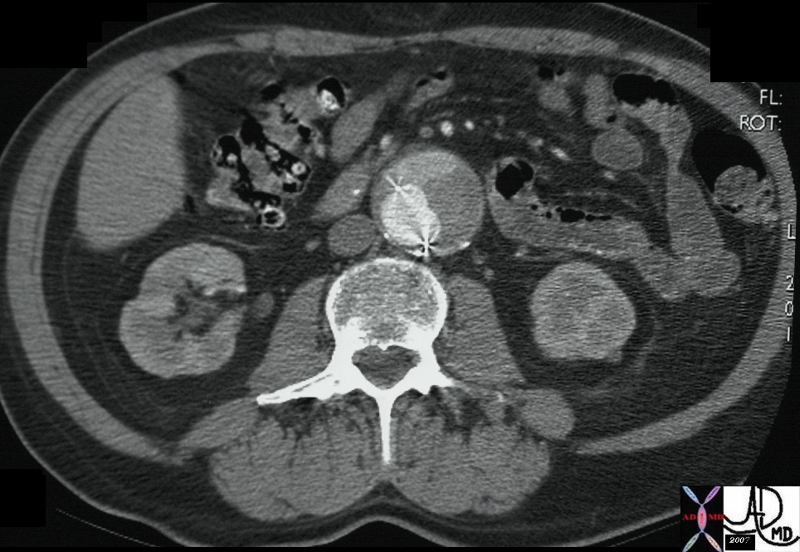
Stent Graft AAA |
| 24285 aorta AAA repair abdominal aortic aneurysm MIT stent graft CTscan Courtesy Ashley Davidoff MD 24286 24284b01 24285 |
Aortic Stent Graft wih Leak |
| 72717 abdomen abdominal aorta AAA s/p stent graft with aortic stent leak leak type 1 CTscan Courtesy Ashley Davidoff MD |
leak from Stent Graft into Sac |
| 24286 aorta AAA repair abdominal aortic aneurysm MIT stent graft aortic sac leak CTscan Courtesy Ashley Davidoff MD 24286 24284b01 24285 |